
Skilled Nursing
Articles

Q&A: Parkinson’s Disease and Parkinson’s Disease Psychosis
May 6, 2024What is Parkinson’s Disease (PD)?
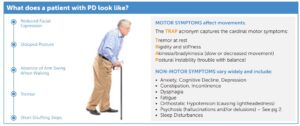
PD is a progressive neurologic movement disorder characterized by motor and non-motor symptoms.
How common is PD?
PD is the 2nd most common neurodegenerative disease, with ~1 million people living with PD in the US alone. 90k new cases are diagnosed each year. The disease is ~1.5x more prevalent in men than women and the primary risk factor for PD is age. 5.2% of LTC residents have a PD diagnosis.
What causes PD?
The precise cause of PD is still unknown. Research suggests both genetic and environmental factors may contribute to disease development. What is known is that loss or impairment of brain nerve cells, specifically dopamine-producing neurons in the brain region known as the substantia nigra, is key to the pathophysiology of this disease. The dopamine neurotransmitter is important to regulating movement patterns, and this is why many PD treatments target increasing brain dopamine levels.
How is PD treated?
It is important to help residents understand that, since PD is an enduring disease, current pharmacologic and nonpharmacologic treatments are not curative and are designed to manage symptoms and maintain ADLs. Because PD is a progressive disease, treatment requirements may change over time. Managing expectations and patient outlook is critical.
Nonpharmacologic approaches to managing PD may include expanding a resident’s interdisciplinary team to include ancillary services to promote regular exercise and daily activity (physical and occupational therapy), healthy diet (dietetics), and therapy to manage changes in speech or swallowing abilities (speech language pathology).
Pharmacologic treatments primarily target the major motor symptoms of PD with multiple classes of medications available to increase brain dopamine levels through distinct mechanisms of action. As PD progresses, a resident’s regimen may be titrated up to maximize individual drug dosages and to include medications across different classes that can produce additive or synergistic effects. The mainstay of motor symptom therapy is established around carbidopa-levodopa. Pharmacologic treatments are also available for non-motor symptoms, such as droxidopa for neurogenic orthostatic hypotension, rivastigmine for dementia associated with PD, and pimavanserin for PDP.
What is Parkinson’s Disease Psychosis (PDP)?
Psychosis is a significant non-motor symptom associated with PD that results in patients experiencing hallucinations and/or delusions. Together, these significant symptoms warrant their own term – Parkinson’s Disease Psychosis.
How common is PDP?
~50% of people with PD may experience hallucinations and/or delusions over the course of their disease.
What causes PDP?
Psychosis is a potential non-motor symptom of PD itself, as well as a known side effect of the dopaminergic medications used to treat PD motor symptoms.
How is PDP treated?
NUPLAZID (pimavanserin) is the only medication FDA-approved for Hallucinations and Delusions Associated with Parkinson’s Disease Psychosis. This is a unique antipsychotic whose mechanism of action targets key serotonin receptors and avoids the pitfall of other antipsychotics that antagonize certain
dopamine receptors that worsen PD motor-symptoms.
NUPLAZID is typically dosed as one 34mg capsule taken by mouth, once daily, with or without food. It may be taken whole or opened and sprinkled on 1 tablespoon of applesauce for immediate consumption for those with swallowing difficulty. *Consult the product’s package insert for full prescribing
information or speak with your doctor or pharmacist.
